Ukraine’s year of war has produced a generation of women oncologists trained in the West

"Unfortunately, Melitopol and Mariupol remain under occupation. There are practically no doctors there, no resources for treatment. There are patients in those territories, and those patients are abandoned, because the occupying authorities have no interest in helping them."
Over the past year, dozens of Ukraine’s female oncologists, who—unlike draft-age men—aren’t restricted from leaving the country, have been receiving training in Western countries, including the United States.
After they return, these women will be poised to take leadership roles in their country’s oncology system, said Andriy Beznosenko, chief of the Division of Surgical Oncology of Abdominal Tumors at the National Cancer Institute of Ukraine in Kyiv and president of the Ukrainian Society of Clinical Oncology.
“Already, many female doctors have gone through internships and come back,” Beznosenko said to The Cancer Letter. “For us, this is an investment in the future, because these physicians return with better training, more up-to-date, and better prepared to improve medical processes at the core of the institute.”
“We can’t directly measure this today, but we are able to say that people are returning with a new perspective, with new impact, which puts them in a position to influence the routine functioning of their departments,” Beznosenko said. “We’ve had quite a few physicians leave for internship training outside the country, but these were usually two-week internships, and now we are talking about two- and three-month internships.”
“But it’s more meaningful, more in-depth. And we are not talking about a small number, but about dozens of physicians.”
Beznosenko, who until recently served as chief medical officer of Ukraine NCI, spoke with Darya Kizub, a hematology and oncology fellow at MD Anderson Cancer Center, who was born in Kyiv and moved to the U.S. at a young age.
Kizub is also director of medical oncology at Global Medical Knowledge Alliance, a non-profit focused on improving cancer and trauma care in Ukraine and globally.
Beznosenko and Kizub spoke in Russian. Their conversation was translated by Paul Goldberg, editor and publisher of The Cancer Letter.
Beznosenko said the volume of patients at his institution has been high in recent months, causing long wait times for surgery and radiation therapy.
“For the first three months [of the war], there were very few patients, because everybody went abroad, but since July, we have had a very large volume, because of resettlement from the occupied territories and regions adjacent to the frontlines,” he said.
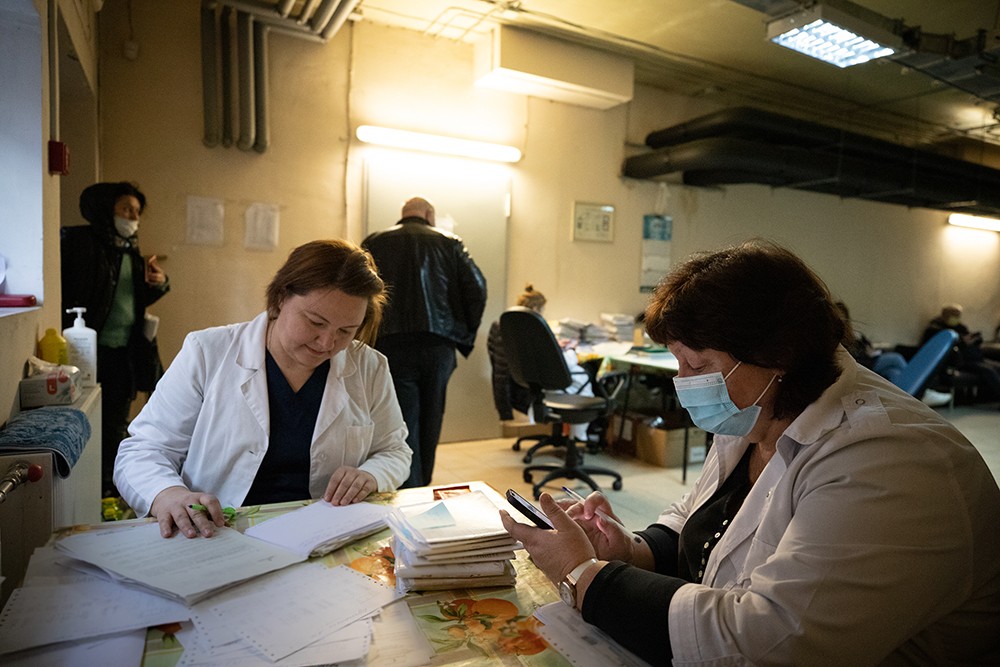
All photos by Oleksiy Samsonov; Kyiv, March 2022
Because of delayed diagnoses, the proportion of patients diagnosed with stage 4 diseases has been going up. “Access to the clinic was disrupted for a couple of months, and by the time they sought help from oncologists, the disease had advanced to a late stage,” Beznosenko said.
Aid groups have been providing drugs and supplies, but shortages persist. Also, clinical trials funded by commercial sponsors haven’t come back, even though NCI is urging companies to return.
“We are trumpeting on all media platforms that new studies should be initiated, because we do have patients,” Beznosenko said. “Alas, for whatever reasons, the sponsors aren’t initiating studies and aren’t starting accruals.”
Julie Gralow, executive vice president and chief medical officer of the American Society of Clinical Oncology, said Ukraine’s oncologists have been able to meet the challenges of the war while also improving the level of professional training of oncologists.
“What impresses me the most during this time of war is that oncologists in Ukraine have not only have worked incredibly hard to assure that their patients receive the best possible care in a time of conflict, but that they have identified and taken advantage of opportunities that arose as part of the crisis that will ultimately, in the long-term post-war, strengthen the oncology workforce and improve the quality of cancer care,” Gralow said to The Cancer Letter.
“This includes training opportunities for female Ukrainian cancer clinicians abroad who will return with new perspectives that will impact cancer care in Ukraine (males not being permitted to leave the country due to possible need for conscription),” Gralow said. “The optimism and resiliency of the Ukrainian people, and their ability to keep their eye on building for a better future post-war, is truly amazing.”
Gralow, a breast cancer expert and a global oncologist, has been working with her Ukrainian colleagues and patient groups for over 25 years (The Cancer Letter, March 4, 2022).
Darya Kizub: How has your work and the work of the National Cancer Institute changed over the past year? What has been most helpful in helping you treat oncology patients?
Andriy Beznosenko: For the first three months, there were very few patients, because everybody went abroad, but since July, we have had a very large volume, because of resettlement from the occupied territories and regions adjacent to the frontlines.
Meanwhile, the resources, medicines, supplies, and personnel have not increased.
The queue for surgery has become longer—two to three weeks. For radiation therapy the wait time is now at one month. The wait times used to be half what they are today.
Drugs have become scarce. Now we have more patients, and patients are having to pay for drugs with their own money, which we see is having an adverse psychological effect. These are patients who have had to leave their homes. Now they must also pay for their treatment. Our partners have been helping us. Mostly, help comes from the diaspora in Portugal, USA, and Great Britain.

This aid comes from the diaspora of physicians who are working in those countries. Their humanitarian aid is now measured in millions of dollars, and it comes in the form of grant money and funding for projects. For example, Natalya Kovalchuk (Stanford School of Medicine) obtained $40,000 from UICC from the radiation therapy department of the Kherson Oncology Center and National Cancer Institute.
Also, an association of Ukrainian doctors in Great Britain is sending us a container full of supplies for surgery every two months. And our Ukrainians who live in Silicon Valley have been helping us—and are continuing to help us—with chemotherapy.
Once a month, they send us enough chemo agents that we are able to feel the impact of this aid at the institute. What else has changed?
We need to mention HUG, Heal Ukraine Group, a group that is helping train our physicians in the United States and Australia. Already, many female doctors have gone through internships and come back.
For us, this is an investment in the future, because these physicians return with better training, more up-to-date, and better prepared to improve medical processes at the core of the institute.
We can’t directly measure this today, but we are able to say that people are returning with a new perspective, with new impact, which puts them in a position to influence the routine functioning of their departments.
We’ve had quite a few physicians leave for internship training outside the country, but these were usually two-week internships, and now we are talking about two and three-month internships.
But it’s more meaningful, more in-depth. And we are not talking about a small number, but about dozens of physicians.
And that is, dozens have already done internships. In what specialties?
AB: Radiation therapy, surgery, chemotherapy, medical physics, colorectal surgery, pancreatic surgery—these are the major specialties.
What about clinical studies? Do you have any ongoing clinical studies, or do you have time for that?
AB: Commercial clinical trials have stopped because of the war. The sponsors aren’t recruiting new patients and aren’t initiating studies.
We are trumpeting on all media platforms that new studies should be initiated, because we do have patients. Alas, for whatever reasons, the sponsors aren’t initiating studies and aren’t starting accruals. Those patients who were enrolled in studies are finishing out their treatment and are provided with everything they need.
There are no new commercial studies, though non-commercial clinical research goes on. People are writing their PhD dissertations in their fields, too.
There have even been public defenses of PhD dissertations during the war—successful ones. In December, Olena Samokhvalova, a onco-gynecologist, successfully defended her dissertation. We are restoring both clinical and scientific structures.
Because of the war, it’s difficult to collect data, because the clinics that are functioning are very busy, which makes it very, very difficult for them to collect data. We are now expecting to update cancer incidence for 2022, hoping to get it completed in late February or early March.
We realize that the war greatly affects this—that we will get a greatly understated number of patients receiving their primary diagnosis since many of them immediately went abroad for treatment, without registering in Ukraine. Many patients, in the frontline areas, have not been able to go to doctors—they have a different prevalence, as it were. But we await this information and once it’s in, we’ll figure out how to interpret it and how to respond.
Are you seeing more patients present with late-stage disease?
AB: Yes—unequivocally. It started in 2020, the two years of COVID, when we saw fewer patients showing up, and in 2021, patients were coming in with more advanced disease. With some diseases—including lung cancer, pancreas, and colon—every third patient who comes through the door has stage 4 disease. That’s a lot. The same thing happened during the war.
During the war, it was exactly the same, because people were abroad, or displaced. Access to the clinic was disrupted for a couple of months, and by the time they sought help from oncologists the disease had advanced to a late stage.
By that point they are symptomatic… Andriy, tell me, how can people—ordinary physicians, oncologists—help you in your work? You’ve described some initiatives that have helped. If someone wants to help in some way, what can they do, and through which organizations?
AB: Well, first, on the National Cancer Institute’s website there are tabs on the for those who want to help financially. And second, there are civic patient organizations, including Inspiration Family and Athena, Women Against Cancer, that collect funds that are targeted specifically for cancer patients, as opposed to the cancer center.
And as a doctor, I see my niche as encouraging our women physicians to get education abroad, so they are putting this time to good use and receiving a good foreign education.
Over the past year, is there any story about your work, or your colleagues, or maybe a patient story that you most remember and that you’d like to share?
AB: There is no shortage of stories from the start of the war, when we had 400 patients on Feb. 24, and how we were discharging them; and when children in pediatric oncology were living in our basement for almost two weeks after bone marrow transplantation, and how we evacuated them.
There were situations where our patients went to see doctors abroad, and we received feedback that we provide high quality care, which inspired us to work even harder. We had funny cases, including one when a patient I had operated on showed up to seek a consultation from my friend and colleague Nelya Melnitchouk in Boston.
My colleague consulted my patient, and both the patient and the physician were displaced persons. Where is Kyiv? Where is Boston? Where are the patients? What’s the distance there—7,000 kilometers or more?
Yes, the world got a little smaller. Tell me, is there anything else that you would like to say to our fellow oncologists in other countries about oncology in Ukraine, what’s most needed, and how you see oncology in Ukraine developing now and after the war.
AB: First, thank you for supporting our trainees. Oncologists and other doctors, particularly in United States, Canada, the European Union helped in training our oncologists.

Some opened their homes and hosted them, so people wouldn’t have to pay rent and other expenses during their internship. This is very valuable, so thank you very much for that.
Also, thank you to those professional societies that have stopped all communication—both public and non-public with doctors in the Russian Federation as a result of this aggression. Unfortunately, not all European professional societies have done this, but almost all organizations in the US have.
"We can’t directly measure this today, but we are able to say that people are returning with a new perspective, with new impact."
I would like to point out that the oncology service in Ukraine has survived the test of the war. All clinics have been functioning and continue to function. Two clinics—Chernigov and Kherson—that were at one point under occupation have reopened.
Unfortunately, Melitopol and Mariupol remain under occupation. There are practically no doctors there, no resources for treatment. There are patients in those territories, and those patients are abandoned, because the occupying authorities have no interest in helping them.
I would like this year to be the year of victory, so we could return our territories so that finally the oncological service will return to high effectiveness and work at a high-enough level.
War changes people in many ways. It changes social structures, too.
What’s your vision of the future? How do you see the development of oncology in Ukraine. It would seem the training of women who had gone abroad to receive training would have an impact.
How do you rebuild a healthcare system? Do you rely on the help from partners in other countries, or will doctors in Ukraine add something of their own?
AB: It should be clear that change should be initiated by Ukrainian doctors and health systems experts. For starters, we should keep in mind that we need to rethink the financing of oncology services, because today we operate—and have in the past operated—under the weight of a colossal deficit.
There are no funds for treatment.
Now, as in the past, patients have to buy some of the medicines and surgical supplies with their own funds—as they have in the past.
This inflicts great financial toxicity.
There are modern protocols, methods of monitoring compliance, assessment of the quality of care.
It’s clear that Ukraine should open itself to the world not only in terms of war, but also in terms of medicine. We should demonstrate that we have competent and professional doctors who are able to provide treatment, analyze data, and publish scientific works.
I think these contacts, which have emerged during the war, will help bring oncology to a new level.